
Tylent Insight
Welcome to the Lyvra Community Tech Blog

From Automation to System Design: Why Incremental Robots Are Not Enough
Automated i.v. compounding robots work—but they rarely transform the process around them. Most platforms replicate manual workflows inside robotic enclosures, preserving serial mechanics and human-dependent steps. The literature shows that these architectural choices create hard limits on throughput, scalability, and risk reduction. Incremental improvements refine machines, but do not change the system. Real progress begins when compounding is redesigned as an end-to-end automated process rather than a sequence of robotic tasks.

Gravimetric Control: Why the De-Facto Standard Is Reaching Its Limits
Gravimetric verification transformed automated i.v. compounding by improving traceability and reducing operator error compared to manual volumetric dosing. Yet from an engineering perspective it also imposes structural limits. In most systems, weighing occurs only before and after dosing, in mechanically noisy environments, making real-time monitoring impossible and turning verification into a retrospective pass/fail check. The next step for automation is not to abandon gravimetry, but to complement it with sensing and control technologies that measure and correct dosing in real time.
End-to-End by Design: Why Partial Automation Fails at the System Level
Most automated i.v. compounding systems stop where the robot stops. Everything before and after is labeled “workflow.” But that is exactly where risk, variability, and hidden costs accumulate. End-to-end automation is not a feature—it is a systems requirement.

From Automation to Care Delivery: Why the System, Not the Device, Matters
Automation has improved many steps of IV compounding—precision dosing, material handling, contamination control. But decades of experience show a clear lesson: technology improves outcomes only when it is designed as part of a broader care delivery system.
Devices optimize individual steps.
Systems ensure that therapy reliably reaches the patient.
When automation stops at the device boundary, fragmentation remains: manual coordination, duplicated safety controls, and pressure shifting between pharmacy and clinical staff. What matters clinically is continuity—from prescription to administration—under real operational conditions.
The next evolution of compounding automation is therefore not simply better machines, but systems designed to coordinate processes, absorb variability, and support care delivery end to end.
Orchestrated Intelligence: Why Automation Without Control Is Not Enough
In i.v. compounding, automation has greatly improved the execution of individual tasks—moving materials, transferring liquids, verifying doses. Yet as systems grow in scale and variability, the real challenge shifts from execution to coordination.
Workflows must constantly adapt to urgent doses, variable preparation times, and unexpected interruptions. In many systems, these decisions still rely on human intervention.
The next step is not simply more automation, but orchestration: systems capable of coordinating processes, balancing workloads, and responding intelligently to change.
Automation performs tasks.
Orchestration makes the system work.

Designing for Parallel Processing: Why Throughput, Safety, and Robustness Converge
In i.v. compounding automation, performance ceilings are often treated as technological limits. In reality, they are architectural. Serial robots force materials, tasks, and decisions to wait their turn, making throughput fragile under real-world variability. Parallel system design removes this constraint, allowing operations to proceed independently and continuously. When processes stop waiting, throughput, safety, and robustness begin to converge.

Human Factors Don’t Disappear: How Automation Still Depends on People (and Why That Matters)
i.v. compounding automation is often described as a way to remove the human factor. In reality, people remain deeply embedded in the workflow—preparing materials, loading components, resolving exceptions, and finishing products. The literature shows that these interactions frequently occur at the most fragile points of the process. Automation reduces handling, but system safety still depends heavily on human reliability.
The Serial Trap: Why Most i.v. Compounding Robots Hit a Performance Ceiling
Across automated IV compounding platforms, a common design pattern emerges: a central workspace served by one or two robotic arms executing tasks sequentially. This architecture places a hard ceiling on scalability. As variability increases, serial workflows amplify delays, corrections, and waiting times. The result is a system that performs well in narrow scenarios but struggles to match the parallel nature of real pharmacy demand.

Semi-Finished Products, Persistent Risk: When Compounding Stops Too Early
IV compounding automation has made mixing safer and more consistent. But most systems still stop too early, delivering semi-finished products that require manual finishing before administration. Every additional handling step—spiking, connecting, priming—reopens the system to exposure and variability. Until automation closes the entire preparation loop, safety gains remain incomplete.

Needles, Coring, and Aerosols: Why Legacy Interfaces Still Drive Risk in IV Compounding
Automation has improved many aspects of i.v. compounding, yet the interfaces connecting drugs to the system remain largely unchanged. Needles, spikes, and perforating access devices are still widely used across automated platforms. The literature shows that these interfaces can generate particulates, aerosols, and micro-leakage during routine operations. As automation scales, the risks associated with these legacy interfaces can become amplified rather than reduced.

Aseptic Technique Beyond the Buzzwords: “ISO 5” Is Not Enough
Automated compounding systems routinely meet sterility expectations, with negative media fills and successful microbiological validation. Yet the literature shows that aseptic risk is not eliminated—it is redistributed. Loading interfaces, non-sterile components, and airflow shadow zones introduce vulnerabilities that ISO 5 classification alone does not address. True aseptic robustness depends not only on room classification but on the continuity of first air and the design of the entire process.

Infusion Sets and Spiking: The Unautomated Step That Undermines Safety
Automation has transformed many aspects of IV compounding, reducing operator contact with hazardous drugs during preparation. However, the attachment of infusion sets—spikes, pigtails, and administration lines—remains largely manual in current workflows. This final step reopens the system to contamination risks and occupational exposure, undermining part of the safety gains achieved earlier in the automated process. In practice, automation frequently stops just before the therapy is fully completed.

Why Throughput Numbers Mislead: Productivity Depends on the Workflow, Not Just the Robot
Throughput figures—doses per hour, preparations per shift—are widely used to evaluate i.v. compounding robots. But the scientific literature shows that productivity is not a property of the robot itself. It emerges from the entire workflow: preparation, logistics, supervision, and post-processing. When these factors are ignored, throughput numbers can be deeply misleading.
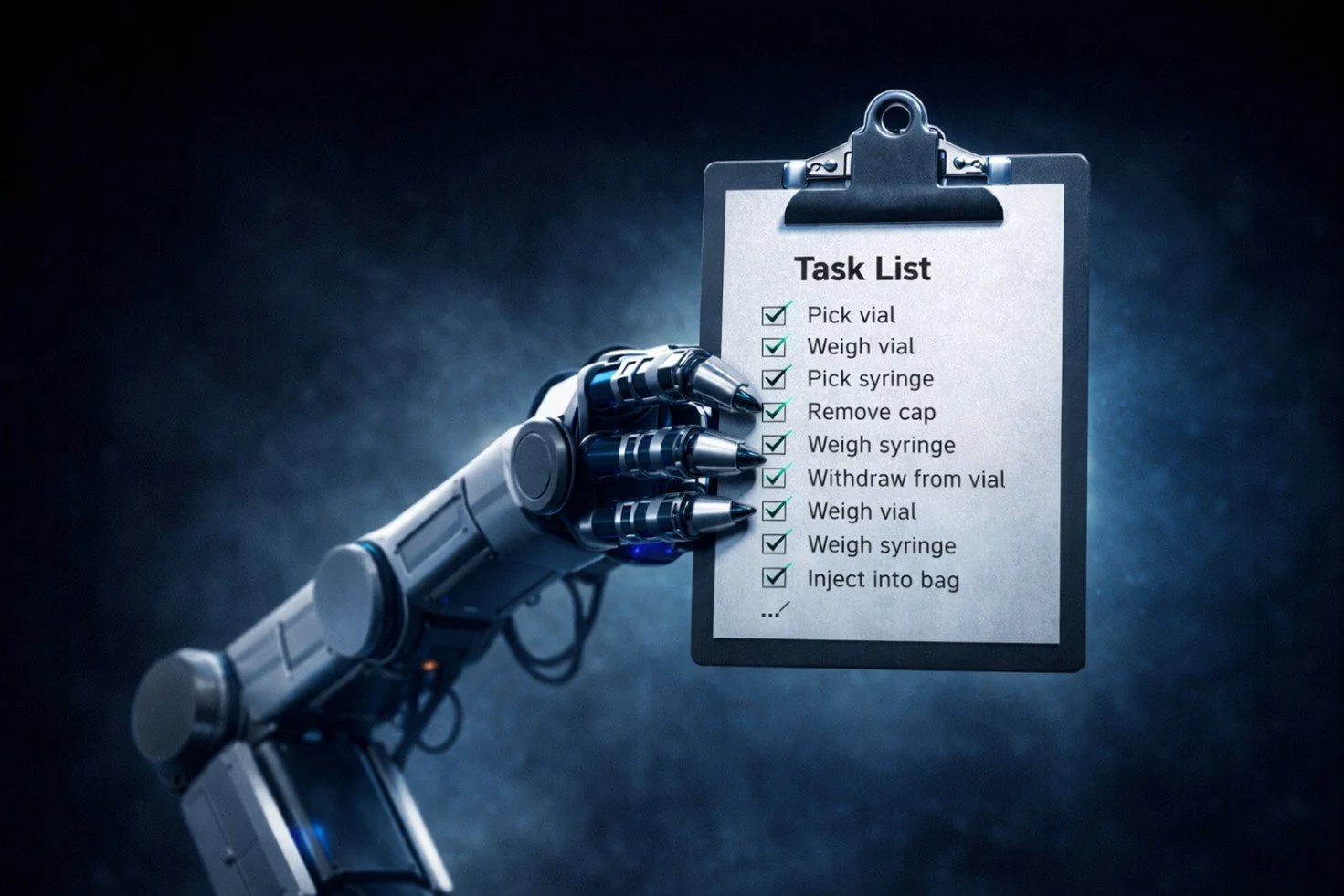
The Hidden Bottleneck: When a Robotic Arm Becomes the System Limiter
In many IV compounding systems, the real bottleneck isn’t software or sensing, but architecture. When a single robotic arm performs every step, the entire workflow becomes serial, turning that actuator into a mechanical choke point. The result: as variability increases, cycle times grow and productivity drops. The future of automation is not simply a better robot, but architectures built on parallelism, orchestration, and scalable workflows.

Are There Really “Generations” of I.V. Compounding Automation?
i.v. compounding automation is often described in “generations,” suggesting major technological leaps. In reality, most systems share the same core architecture: robots that replicate manual aseptic work inside an isolator while much of the surrounding workflow remains manual. The result is incremental improvement, not true transformation. When variability increases, throughput often approaches manual levels. A real next generation will require rethinking the workflow itself, designing automation around parallel processes and end-to-end control rather than simply imitating manual practice.